Absent or limited motion of the left corner of the mouth is demonstrated in the child.
Popular Search Terms
Research & Innovation
Innovative treatment
In newborn infants, protection of the eye is of utmost importance. Keeping the eye well-lubricated is usually sufficient to protect it. When this fails, the eyelids can be partially closed in an operation called tarsorrhaphy.
For restoration of smile and oral competence, two main methods are available: static slings and functional muscle transfers.
- Static slings use the patient's own tissues to improve symmetry and function around the mouth and the eye.
- Dynamic muscle transfers can be done with local or distant muscles to help the patient smile and restore lip position.
- In suitable candidates, the ideal way to restore smile is using a distant muscle transfer through microsurgical techniques. See the illustration of a distant muscle transfer below.
Image

Image
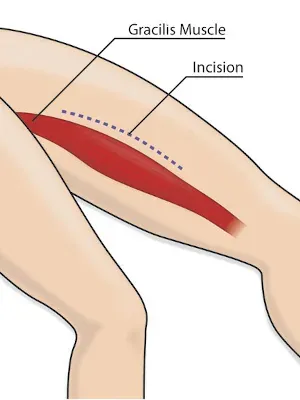
The gracilis muscle is removed through a five-inch incision in the upper inner thigh. Although a scar remains, there is no loss of function in the leg.
Image
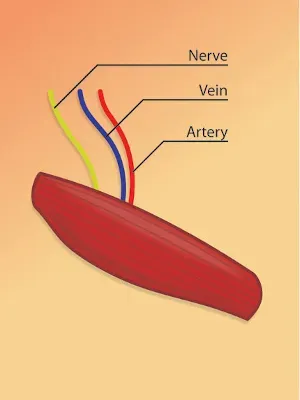
The muscle is removed along with the artery (red line), vein (blue line), and nerve (yellow line) that supply it. The muscle is then tapered to fit each child’s face individually.
Image

A second team of surgeons will use the “facelift” type incision to expose the area into which the muscle will be transferred.
Image
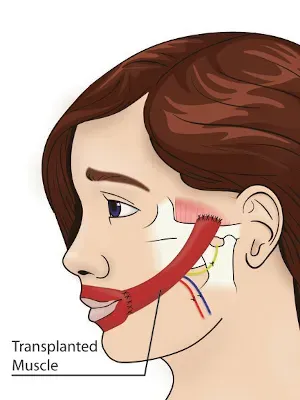
The muscle is then connected to the facial artery and vein and a motor nerve. The muscle is held in position using non-dissolving anchoring sutures.
Image
All incisions are closed with dissolving sutures.