Contact Us
Department of Neurosurgery
7:00 am - 8:00 pm
The Movement Disorders Program at Boston Children’s Hospital provides specialized, multidisciplinary care for children with dystonia and other rare, complex movement disorders. As part of this care, we offer deep brain stimulation (DBS), a surgical treatment that can help improve symptoms, comfort, and quality of life. DBS may be recommended for certain genetic forms of dystonia and for children whose symptoms don’t improve with medication alone or significantly interfere with daily activities and require care from multiple specialists.
Our pediatric DBS team brings together experts in neurology, neurosurgery, genetics, rehabilitation, and other specialties to carefully evaluate each patient and support families through every stage of care — from the first consultation through long-term follow-up.
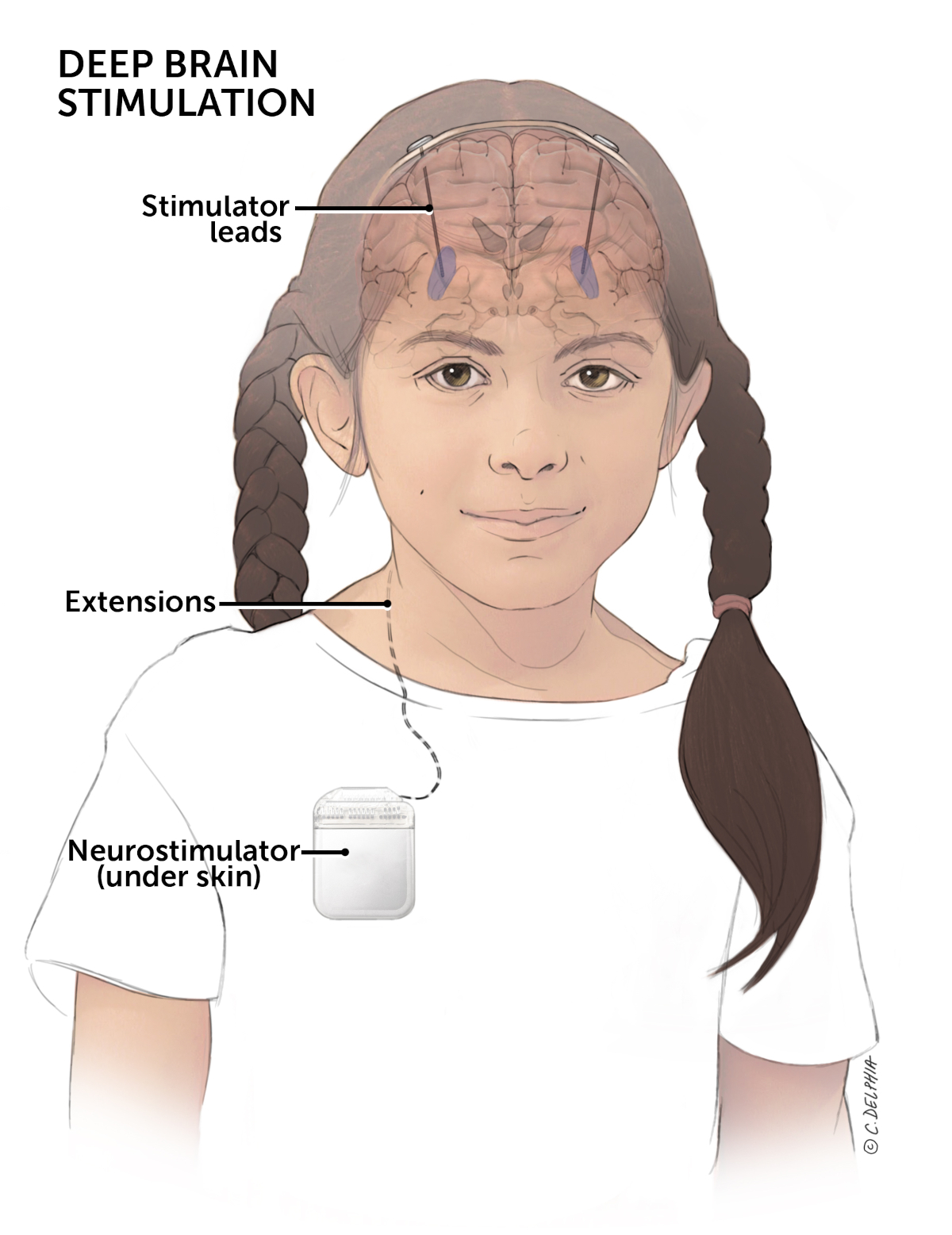
Deep brain stimulation (DBS) is a surgical treatment that uses gentle electrical signals to regulate abnormal brain activity that causes involuntary movement. In some children with movement disorders, faulty brain circuits send excessive signals to the muscles, leading to stiffness, unusual postures, and difficulty moving. DBS delivers adjustable stimulation to specific areas of the brain to calm these signals and reduce symptoms. While not a cure, DBS can significantly improve symptoms and quality of life for some children.
Improvement with DBS typically happens gradually over weeks to months as stimulation settings are adjusted.
For children with movement disorders, electrodes are generally placed in the globus pallidus internus (GPi), a part of the brain that helps control movement. After surgery, stimulation settings — such as intensity, pulse width, and frequency — are customized and adjusted over time to maximize benefit and comfort.
Before DBS, children are evaluated by our multidisciplinary team, which may include:
Advanced imaging and diagnostic testing help determine whether DBS is likely to be beneficial and to help guide surgical planning.
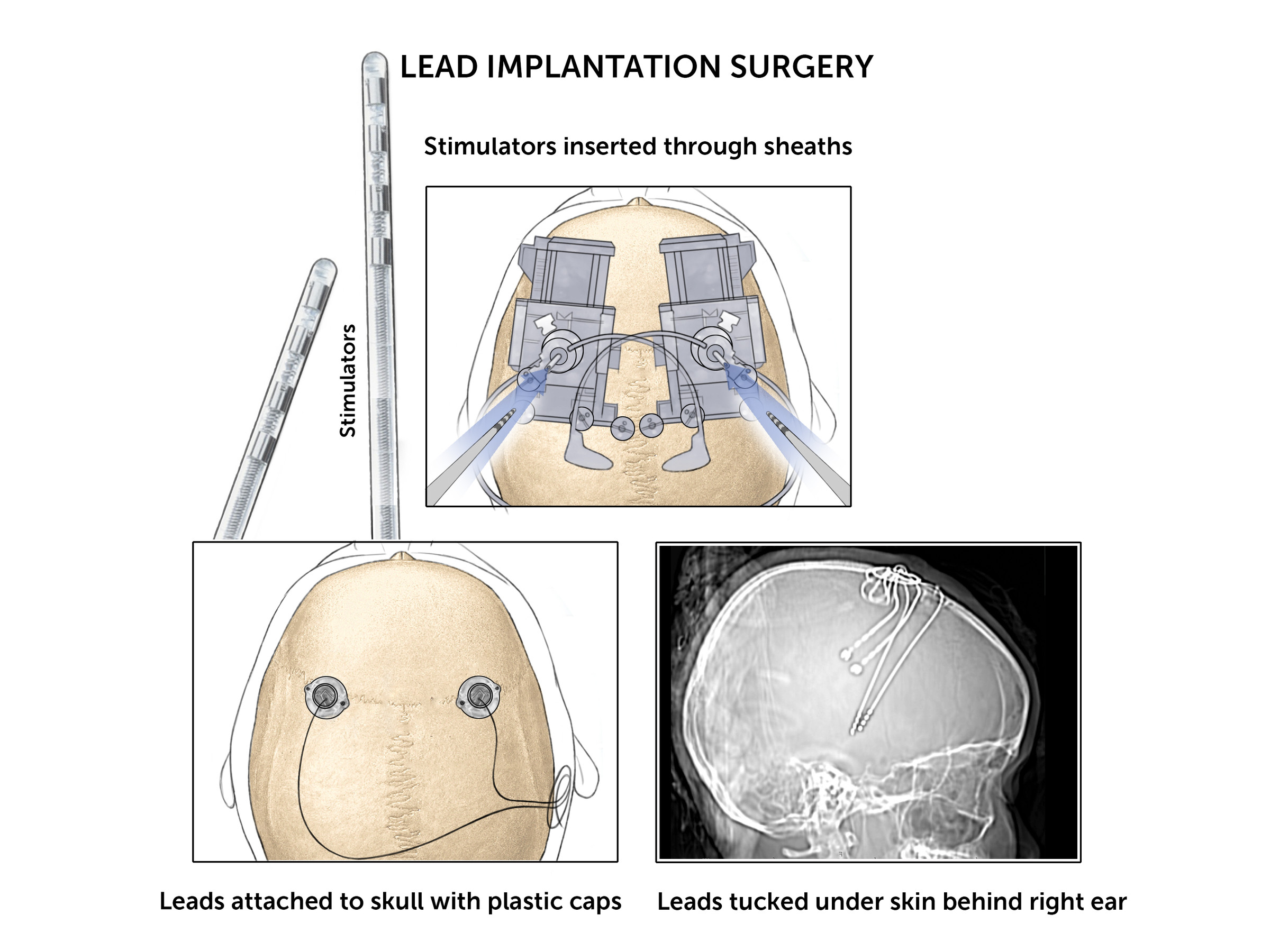
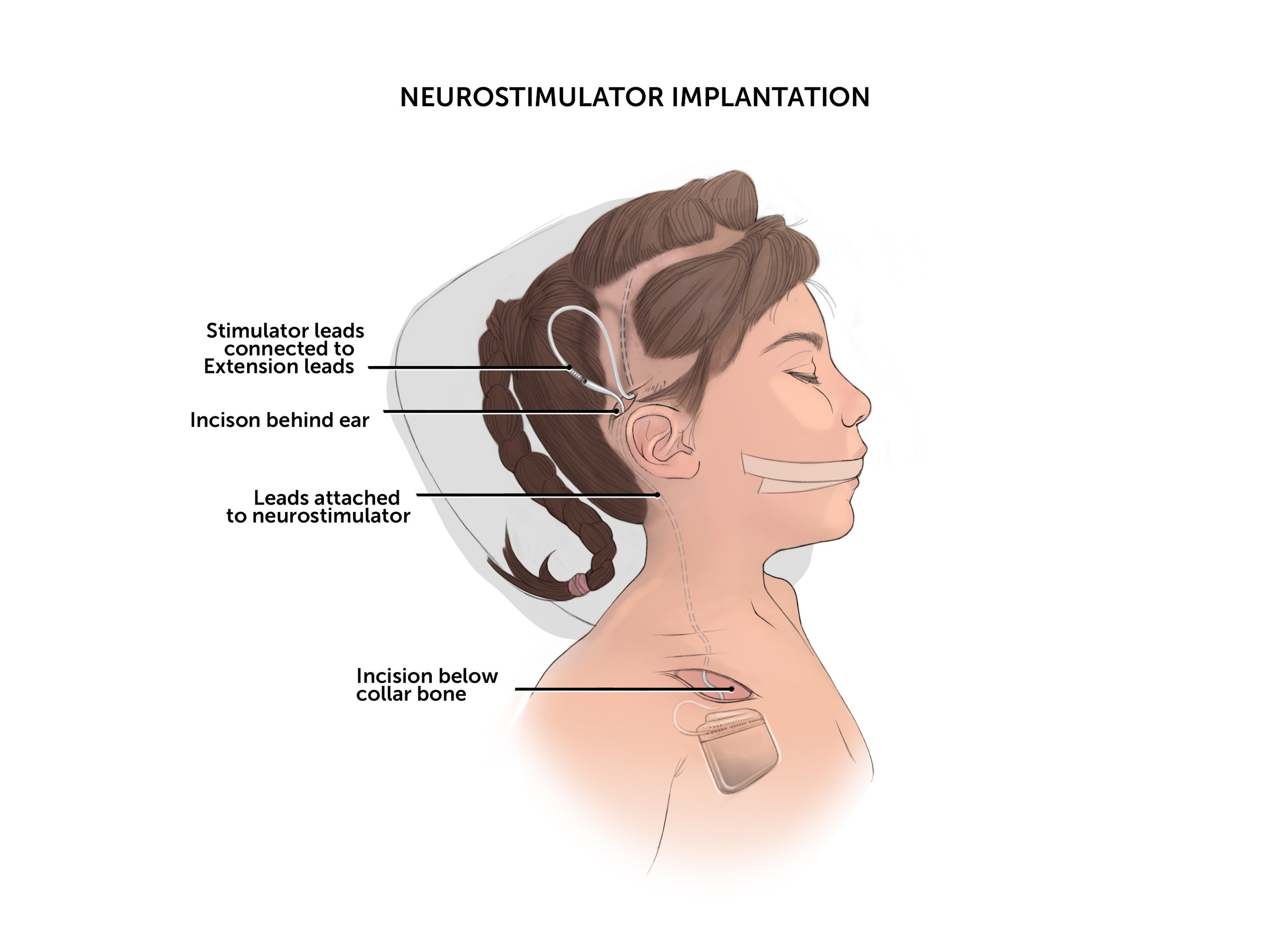
The procedure is typically performed in one stage. This involves:
Post-op, there is an in-hospital stay for surgical recovery followed by initial programming performed in an outpatient setting.
The DBS device can be programmed and adjusted using a wireless controller. Families also receive a monitoring device to use at home.
After surgery, children are closely monitored with regular follow-up by our team. DBS therapy requires periodic visits to adjust stimulation settings as the child grows and symptoms change, helping ensure the best possible benefit.
Click on images below to enlarge.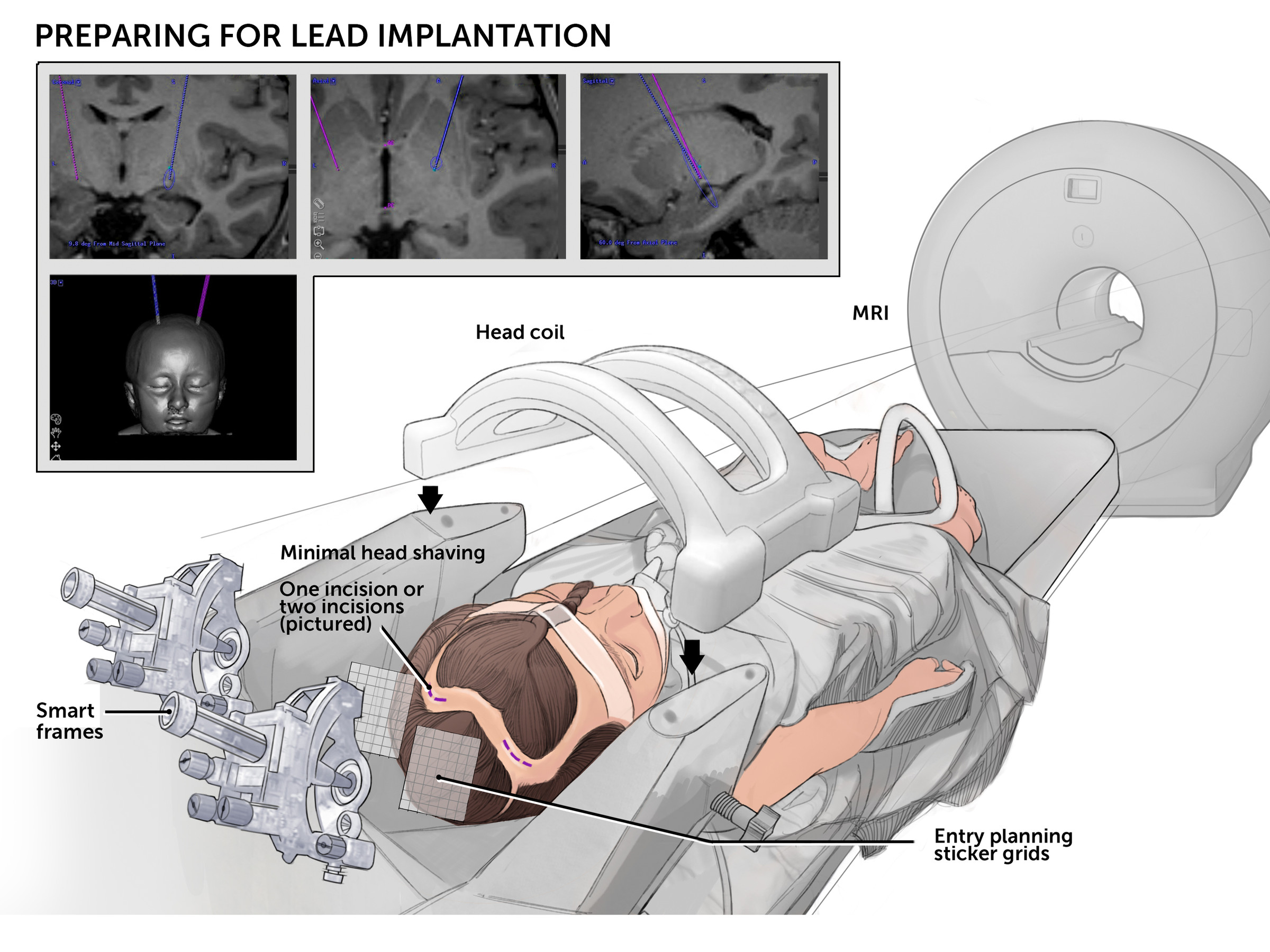
Children with significant movement symptoms may benefit from DBS. Because indications for DBS continue to expand, our team evaluates every child individually, recognizing that DBS may help different children in different ways.
DBS is generally considered a lower-risk procedure, but as with any surgery, there are potential risks. These may include:
Your child should not feel the stimulation once the settings are optimized.
Battery life depends on the stimulation settings and the type of device. Current rechargeable systems last many years.
Yes, DBS is adjustable and reversible.
Referring a patient
We welcome referrals for children with genetic or complex movement disorders who may be candidates for DBS. Please contact the Movement Disorders Program to discuss eligibility and required records.
DBSMatchMaker
We developed DBSMatchmaker.com for specialists caring for children with monogenic movement disorders who are considering or implanting DBS. This online platform supports peer-to-peer collaboration, shared learning, and data-informed decision-making in rare and complex cases.