Nemaline Myopathy | Overview
Nemaline Myopathy is a condition characterized by proximal muscle weakness, delayed motor milestones and occasionally respiratory insufficiency and feeding problems (Sewry, Laitila, and Wallgren-Pettersson 2019). The condition is identified by muscle biopsy which shows distinctive rod-shaped structures in muscle cells (Conen, Murphy, and Donohue 1963; Shy et al. 1963). There is a wide spectrum of severity and classically patients have been divided into 6 groups; “Severe” with neonatal respiratory insufficiency, contractures or absent movement, “Intermediate” with a less severe neonatal course but inability to achieve walking or respiratory independence in childhood, “Typical” with onset of weakness in infancy or young childhood and delayed, but reached, milestones, “Mild Childhood/Juvenile” onset with minimal weakness and no major respiratory involvement, “Adult onset” which presents with rapidly progressive weakness in later adulthood, and a group labeled “Other” due to unusual features including pronounced distal weakness, cardiomyopathy, ophthalmoplegia or intranuclear rod bodies on microscopic examination (Wallgren-Pettersson and Laing 2000).
Microscopic examination of muscle biopsies often shows accumulation of darkly staining structures called nemaline rods. Electron microscope examination often reveals that these rods are contiguous with abnormal Z-disks (Sewry, Laitila, and Wallgren-Pettersson 2019; Malfatti et al. 2014).
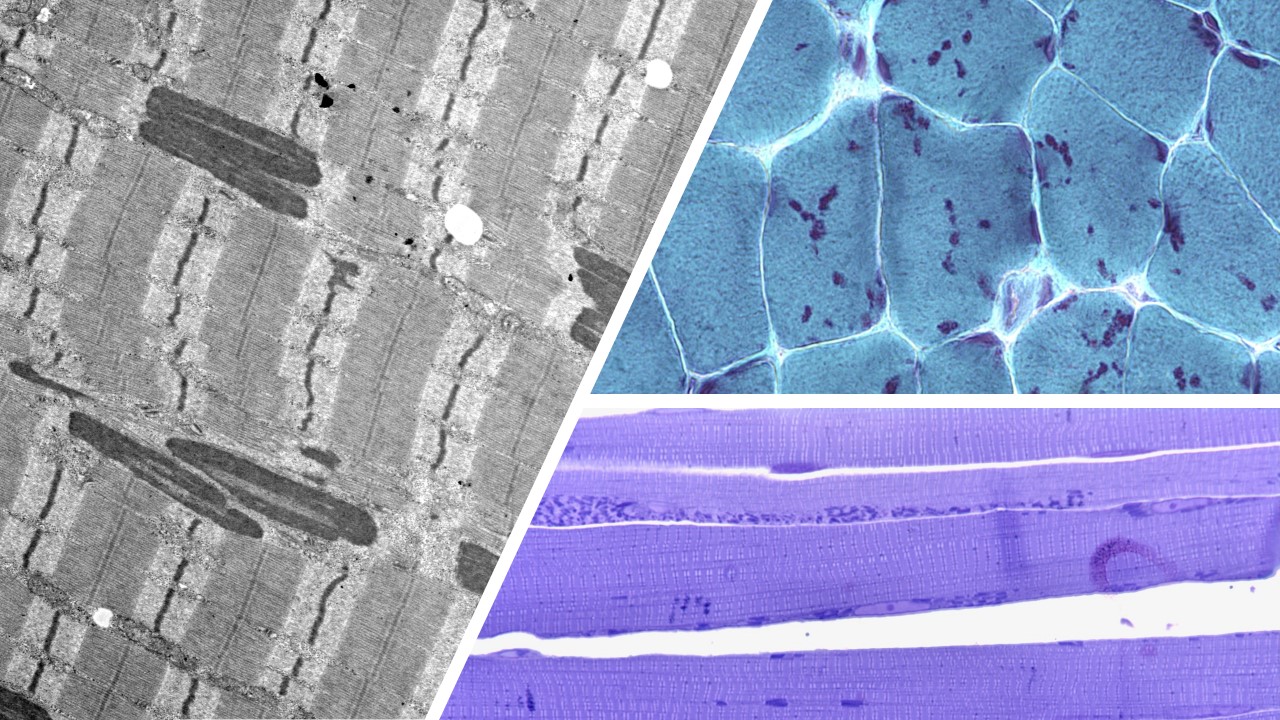
Muscle cells exhibiting the classic dark "nemaline rods" in a few different types of stains.
Our laboratory is interested in studying DNA and muscle tissue samples of individuals with Nemaline Myopathy to provide further insight into the genetic causes of their condition. Identification of these genes could have direct clinical benefit to patients and their families by allowing for specific diagnostic testing such as carrier detection and prenatal diagnosis. Furthermore, understanding the genetic causes of Nemaline Myopathy will increase our understanding of muscle biology and provide insights into future development of specific treatments and therapies.
Genetics
The understanding of the genetic etiology of NM is continuing evolve. To this date 12 genes have been linked to Nemaline Myopathy (ACTA1, CFL2, KBTBD13, KHLH40, KHLH41, LMOD3, MYBN, NEB, TNNT1, TNNT3, TPM2, TPM3). Some show autosomal recessive inheritance, some autosomal dominant (Sewry, Laitila, and Wallgren-Pettersson 2019). Microscopic structures called thin filaments, are in part responsible for the formation of skeletal muscle fibers. The above genes code for proteins that are important in maintaining normal functioning of these thin filaments of the sarcomere, the contractile units of muscle cells. When the sarcomeric architecture and function are disrupted, the force of muscle contraction is decreased leading to weakness (Joureau et al. 2018). It can be difficult to predict the severity of symptoms based on which gene is involved but some connections have emerged. A certain genetic change in TNNT1 seen in the Amish population causes a distinct presentation with severe early onset disease including respiratory failure (Fox et al. 2018). Additionally, changes in KBTBD13 are associated with abnormal slowness of movements and cores in addition to rods seen on muscle biopsy (Sambuughin et al. 2010).
Research
In the Beggs Laboratory, one of our goals is to determine which additional genes and proteins are involved in Nemaline Myopathy. We are also interested in linking the type of genetic change to the Nemaline Myopathy symptoms that can be expected (genotype to phenotype correlation). If you are the parent of a child with Nemaline Myopathy, if you yourself are affected, or if you are the healthcare provider of a patient with nemaline myopathy, you may be able to help us find new genes and proteins associated with Nemaline Myopathy. With the generous help of enough candidate families, we may be able to learn information that will hopefully help us to better understand this disorder, improve diagnosis and develop of new treatments and therapeutic methods.
References
Conen, P. E., E. G. Murphy, and W. L. Donohue. "Light and Electron Microscopic Studies of "Myogranules" in a Child with Hypotonia and Muscle Weakness." Can Med Assoc J 89 (1963): 983-6.
Fox, M. D., V. J. Carson, H. Z. Feng, M. W. Lawlor, J. T. Gray, K. W. Brigatti, J. P. Jin, and K. A. Strauss. "Tnnt1 Nemaline Myopathy: Natural History and Therapeutic Frontier." Hum Mol Genet 27, no. 18 (2018): 3272-82.
Joureau, B., J. M. de Winter, S. Conijn, S. J. P. Bogaards, I. Kovacevic, A. Kalganov, M. Persson, J. Lindqvist, G. J. M. Stienen, T. C. Irving, W. Ma, M. Yuen, N. F. Clarke, D. E. Rassier, E. Malfatti, N. B. Romero, A. H. Beggs, and C. A. C. Ottenheijm. "Dysfunctional Sarcomere Contractility Contributes to Muscle Weakness in Acta1-Related Nemaline Myopathy (Nem3)." Ann Neurol 83, no. 2 (2018): 269-82.
Malfatti, E., V. L. Lehtokari, J. Bohm, J. M. De Winter, U. Schaffer, B. Estournet, S. Quijano-Roy, S. Monges, F. Lubieniecki, R. Bellance, M. T. Viou, A. Madelaine, B. Wu, A. L. Taratuto, B. Eymard, K. Pelin, M. Fardeau, C. A. Ottenheijm, C. Wallgren-Pettersson, J. Laporte, and N. B. Romero. "Muscle Histopathology in Nebulin-Related Nemaline Myopathy: Ultrastrastructural Findings Correlated to Disease Severity and Genotype." Acta Neuropathol Commun 2 (2014): 44.
Morton, S. U., M. Joshi, T. Savic, A. H. Beggs, and P. B. Agrawal. "Skeletal Muscle Microrna and Messenger Rna Profiling in Cofilin-2 Deficient Mice Reveals Cell Cycle Dysregulation Hindering Muscle Regeneration." PLOS ONE 10, no. 4 (2015): e0123829.
Nowak, K. J., G. Ravenscroft, C. Jackaman, A. Filipovska, S. M. Davies, E. M. Lim, S. E. Squire, A. C. Potter, E. Baker, S. Clement, C. A. Sewry, V. Fabian, K. Crawford, J. L. Lessard, L. M. Griffiths, J. M. Papadimitriou, Y. Shen, G. Morahan, A. J. Bakker, K. E. Davies, and N. G. Laing. "Rescue of Skeletal Muscle Alpha-Actin-Null Mice by Cardiac (Fetal) Alpha-Actin." J Cell Biol 185, no. 5 (2009): 903-15.
Ravenscroft, G., C. Jackaman, S. Bringans, J. M. Papadimitriou, L. M. Griffiths, E. McNamara, A. J. Bakker, K. E. Davies, N. G. Laing, and K. J. Nowak. "Mouse Models of Dominant Acta1 Disease Recapitulate Human Disease and Provide Insight into Therapies." Brain 134, no. Pt 4 (2011): 1101-15.
Sambuughin, N., K. S. Yau, M. Olive, R. M. Duff, M. Bayarsaikhan, S. Lu, L. Gonzalez-Mera, P. Sivadorai, K. J. Nowak, G. Ravenscroft, F. L. Mastaglia, K. N. North, B. Ilkovski, H. Kremer, M. Lammens, B. G. van Engelen, V. Fabian, P. Lamont, M. R. Davis, N. G. Laing, and L. G. Goldfarb. "Dominant Mutations in Kbtbd13, a Member of the Btb/Kelch Family, Cause Nemaline Myopathy with Cores." Am J Hum Genet 87, no. 6 (2010): 842-7.
Sewry,C. A., J. M. Laitila, and C. Wallgren-Pettersson. "Nemaline Myopathies: A Current View." J Muscle Res Cell Motil 40, no. 2 (2019): 111-26.
Shy, G. M., W. K. Engel, J. E. Somers, and T. Wanko. "Nemaline Myopathy. A New Congenital Myopathy." Brain 86 (1963): 793-810.
Sztal, T. E., E. A. McKaige, C. Williams, A. A. Ruparelia, and R. J. Bryson-Richardson. "Genetic Compensation Triggered by Actin Mutation Prevents the Muscle Damage Caused by Loss of Actin Protein." PLoS Genet 14, no. 2 (2018): e1007212.
Wallgren-Pettersson, C. and N. G. Laing. "Report of the 70th Enmc International Workshop: Nemaline Myopathy, 11-13 June 1999, Naarden, the Netherlands." Neuromuscul Disord 10, no. 4-5 (2000): 299-306.
This page was last updated October 23, 2020.