The first three months of a pregnancy are a critical time for a growing fetus: In addition to many other developments taking place throughout the body, the structure of the mouth and face also begins to take shape.
Around the fifth to sixth week of pregnancy is when the two sides of a baby’s upper lip will fuse together. Sometimes the fusing process does not happen properly which results in the upper lip being split, or cleft.
A child with a cleft lip has a visible separation in the skin of their top lip. This space can be a small hole, or it can be a significant opening that extends from the base of the baby’s nose all the way down to their top jaw and gums.
By the eighth to ninth week of pregnancy, the roof of the baby’s mouth (palate) should be formed. The roof of the mouth is made up of two parts:
- the hard palate, the firm and bony plate hugging the horseshoe-shaped curve of the top teeth
- the soft palate, the flexible, fleshier tissue that spans the back of the mouth
When the development of one or both of these parts is incomplete, the baby has what is known as a cleft palate.
A child can be born with a cleft lip, a cleft palate, or both:
- when combined, affect one in every 700 babies born in the U.S., making them the fourth most common birth defect nationwide
- can be unilateral — involving only one side of the mouth and face — or bilateral, involving both
- are more common in boys than girls
- affect more children of Asian, Latino, and Native American descent — and fewer of African-American descent — than children of other ethnicities
The good news is that babies with a cleft lip and cleft palate are very treatable. Although children with more advanced cases may require assistance in several areas, and may need multiple procedures over time, there are several minimally invasive treatment options available to help them regain a normal appearance and range of functions.
Cleft Lip and Cleft Palate | Symptoms & Causes
The shape and structure of a baby’s mouth and face begin to materialize in the early weeks of pregnancy:
- Around the fifth to sixth week, the two sides of the upper lip fuse together.
- By the eighth to ninth week, the roof of the mouth is formed.
However, when something disrupts one or both of these processes, the result is often condition called cleft lip and/or a cleft palate.
- A cleft lip is a split, or cleft, in the skin of the upper lip. This defect can range in size from a tiny, almost imperceptible hole to a very large opening that includes the top gum and top jaw.
- A cleft palate is an opening in the roof of the mouth. This opening can go through the bony hard palate around the top row of teeth; through the fleshy soft palate at the back of the mouth; or through both parts.
Many children have both a cleft lip and a cleft palate. If the defect only occurs on one side, it is called unilateral. If it involves both sides, the cleft lip and cleft palate is bilateral.
Cleft lip and cleft palate can present a number of challenges for a child, including possible:
- feeding issues
- dental and orthodontic problems
- speech and language difficulties
- hearing impairment
- social and self-esteem challenges
Because cleft lip and cleft palate can vary widely in severity from child to child, treatment options also encompass a broad spectrum. A baby with a very minor, unilateral cleft lip, for example, might only need one procedure, while an infant with a more involved cleft that runs through both sides of his palate may require many different interventions throughout their life into the teenage years or early adulthood.
You can rest assured that — regardless of the extent of your child’s cleft lip and cleft palate — there is plenty of cause for hope: These conditions are very manageable. In fact, thanks to recent advances in diagnostics and care, treatment can often shortly after birth.
Here at Boston Children’s, our multidisciplinary Cleft Lip and Palate Program is designed to meet the needs of children of all ages and with all variations of cleft lip and cleft palate. No matter your child’s specific circumstances, we are ready to help them — and to include you and your family in the treatment process at every step of the way.
What causes cleft lip and cleft palate?
We know that cleft lip and cleft palate are congenital defects — which means they are present at birth — and that they involve a disruption to the formation of the fetus’s top lip and/or roof of the mouth. However, no one knows exactly why these disruptions take place.
It is believed that cleft lip and cleft palate may be genetic conditions (resulting from an error in the genes). Some children with cleft lip and cleft palate have other family members with the defect, but in most cases, there is no evidence of any family history.
Scientists believe that some instances of cleft lip and cleft palate may happen because of something that affected the mother during pregnancy, including:
- taking certain medications
- using tobacco or alcohol
- vitamin deficiency
- viral illness
Finally, in rare cases, a child’s cleft lip and cleft palate may be related to a syndrome such as Van der Woude syndrome, Stickler syndrome, or Kabuki syndrome.
What are the symptoms of cleft lip and cleft palate?
Nearly all babies with cleft lip and cleft palate are diagnosed at birth (or even before, through prenatal ultrasound) because the defects are readily apparent.
In rare cases, a child may have a cleft palate that only involves her soft palate (the fleshy tissue at the back of her mouth) and isn’t evident on an initial visual exam. The first sign of a problem in these babies is usually difficulty feeding (an inability to latch on to the breast or bottle nipple, or to use consistent suction while nursing).
Frequently asked questions (FAQ) about cleft lip and cleft palate
No. A child can be born with just a cleft lip, just a cleft palate or a combination of both.
At the moment, there is no known way to prevent cleft lip and cleft palate; in order to understand how to prevent these defects, we would first need to understand how and why they occur. Researchers are hard at work on uncovering new insights, but have found no proven cause as of yet.
Some theories suggest that certain steps might contribute to preventing cleft lip and cleft palate, namely:
- undergoing genetic testing and genetic counseling
- avoiding alcohol and tobacco consumption during pregnancy
- increasing the intake of folic acid during pregnancy
No; in fact, there are several types of cleft lip.
The lip, nose and palate can all be involved to varying degrees. The major types of cleft lip are:
- unilateral (occurring to either the left or right of the midline of the face and mouth; for reasons we don’t fully understand, the left side is more commonly affected)
- bilateral (occurring on both the left and right sides)
And there are three subtypes:
- incomplete (only partial fusion of the two sides of the top lip)
- complete (total absence of any fusion)
- asymmetrical (complete on one side and incomplete on the other)
Yes. Your child’s cleft lip can be closed with a surgical procedure. After the operation, your child’s mouth and nose will be near normal in appearance and should function normally.
Most cleft lips are closed before 6 months of age. If your child also has a cleft palate, that will be repaired in a separate operation. Your plastic surgeon will talk to you about the best surgical timing for your child.
No. The palate is composed of two parts, a fleshy, muscular part (soft palate) and a bony part (hard palate). The soft and hard palate can be involved to varying degrees.
Yes. The opening in the hard and/or soft palate is usually closed in one operation, though your child may need more than one procedure depending on his particular circumstances. Your treatment team will outline specific recommendations.
Unfortunately, no. At this time, there are no available tests that can detect the genetic changes responsible for cleft lip and cleft palate.
The chance of having more than one child with a cleft lip and/or cleft palate is different for each family. In general, if there is one affected person in the family with a cleft, the likelihood of having a child with a cleft lip and/or palate is 2 to 5 percent. If there is a second affected person in the family (either another sibling or a parent), the chance of future children having a cleft lip increases to 10 to 14 percent, and the risk of a future child having an isolated cleft palate rises to 8 percent.
Here at Children’s, a geneticist on your child’s cleft treatment team can provide detailed information about your family’s particular situation.
If your infant has a cleft lip only, they should be able to directly breastfeed without any modifications. If your infant has a cleft palate, breastfeeding can be difficult because the baby is often not able to create the suction necessary due to the cleft. Breast milk may still be pumped and provided to the baby via a specialty bottle. Our nurses in the department are experts in feeding infants with clefts and will work with you to find the options that are best for your baby. Learn more in our Diagnosis and Treatments section.
Not necessarily, but it is possible. Children born with a cleft palate often have temporary hearing loss because of fluid in the middle ear and recurring ear infections. This hearing loss may last for a short time, or it may persist for a number of months.
Speech and language development is influenced by a child’s ability to hear well. Your child will undergo her first hearing test early in life, and will be tested again prior to the operation to repair her cleft palate. Her age and developmental level will determine which hearing test method will be used. Children born with cleft palates often need to have ear tubes placed at the time of the cleft palate repair. Learn more in our Diagnosis and Treatments section.
Possibly. Some children with a cleft palate have speech and language delays. These may be related to the temporary hearing loss associated with the cleft palate and middle ear fluid.
Some children exhibit difficulty with speech if their palate is not effectively closing off the nose from the mouth while they are speaking. However, the good news is that most will acquire speech and language skills at a normal pace after the palate is closed and middle ear tubes are placed for drainage. Learn more in our Diagnosis and Treatments section.
If your child has a cleft lip and/or cleft palate, he may be more susceptible to developing cavities. Learn more in our Diagnosis and Treatments section.
If the palate or gum line (alveolus) were affected by the cleft, it is likely that your child will require some form of orthodontic treatment. Learn more in our Diagnosis and Treatments section.
Cleft Lip and Cleft Palate | Diagnosis & Treatments
The first step in treating your child is forming an accurate and complete diagnosis.
How is cleft lip/cleft palate diagnosed?
In most cases, a prenatal ultrasound can detect cleft lip alone or cleft lip and palate as early as 16 weeks into a pregnancy. The diagnosis is then confirmed at birth with a detailed visual assessment and physical examination. In some cases of incomplete cleft lip, the diagnosis cannot be seen on ultrasound and is made for the first time at birth.
Cleft palate can occur alone, without cleft lip. This type of cleft may not show up on ultrasound and may be diagnosed for the first time at birth. At that point, a clinician will perform a comprehensive exam to identify the exact nature of the problem and determine whether the cleft involves the hard and soft palate, or the soft palate only. In a small number of cases, cleft palate is diagnosed on a fetal MRI performed for other reasons, such as a small lower jaw. Infrequently, a minor case of cleft soft palate will not even be seen at birth and will become noticeable later when the infant experiences difficulty feeding.
How we treat cleft lip and cleft palate
Treatment for a cleft lip/cleft palate usually involves reconstructive surgery and several key support services.
The Cleft Lip and Palate Program at Boston Children’s Hospital takes a multidisciplinary team approach to repairing your child's specific cleft and addressing related conditions.
While your child's treatment plan will depend on their individual circumstances — as well as your family's preferences — here are some frequently asked questions about treating cleft lip/cleft palate:
Surgical repair: Cleft lip
Many children with a unilateral complete cleft lip and palate have a large gap between their gums. To move the gums and palate into a closer position, presurgical orthopedics are often recommended. In most cases, this is a Latham-type appliance. A dentist inserts this device in the operating room when a child is around 2 or 3 months old. You will need to turn a small screw on the device to slowly bring the gums together. The device is removed at the time of either lip-nasal adhesion or complete cleft lip repair.
For some children with unilateral cleft lip who have more severe nasal asymmetry, nasal molding may be recommended. A DynaCleft® nasal elevator is an external device that may be started at the first clinic visit. This device slowly rounds and elevates the nasal cartilage to improve nasal shape and can be used with or without a Latham-type appliance.
For some children with a unilateral cleft lip, the first operation recommended is a lip-nasal adhesion. This operation is performed at about 3 months of age, and involves:
- simple closure of the lip
- the first stage of nasal correction
- when possible, closure of the cleft in the upper gum (this procedure is called gingivoperiosteoplasty)
When a single operation is recommended, either for unilateral or bilateral cleft lip, it typically occurs when the child is between 3 and 5 months of age. During this operation, the baby's nasal asymmetry (unevenness in the shape of the nose) is also corrected. A plastic surgeon uses the existing muscle and tissues of your child's lip and nose to close the cleft. Repair of a unilateral cleft lip is performed in the operating room under general anesthesia. Your child will stay in the hospital for one to two nights after the operation.
In children for whom two operations are recommended, the first is lip-nasal adhesion. The second operation is a more comprehensive repair of the cleft lip and correction of the nose. This procedure usually takes place around three months later, at 5 to 6 months of age.
After the operation, your child's lip, nose, and face will be swollen for a few days. The scar may be red for several months. It will take 6 to 12 months for the scar to soften and fade.
Although it will never completely disappear, in time, the scar will become difficult to see. Your child's lip and nose will be nearly normal in appearance after the swelling and scar have subsided.
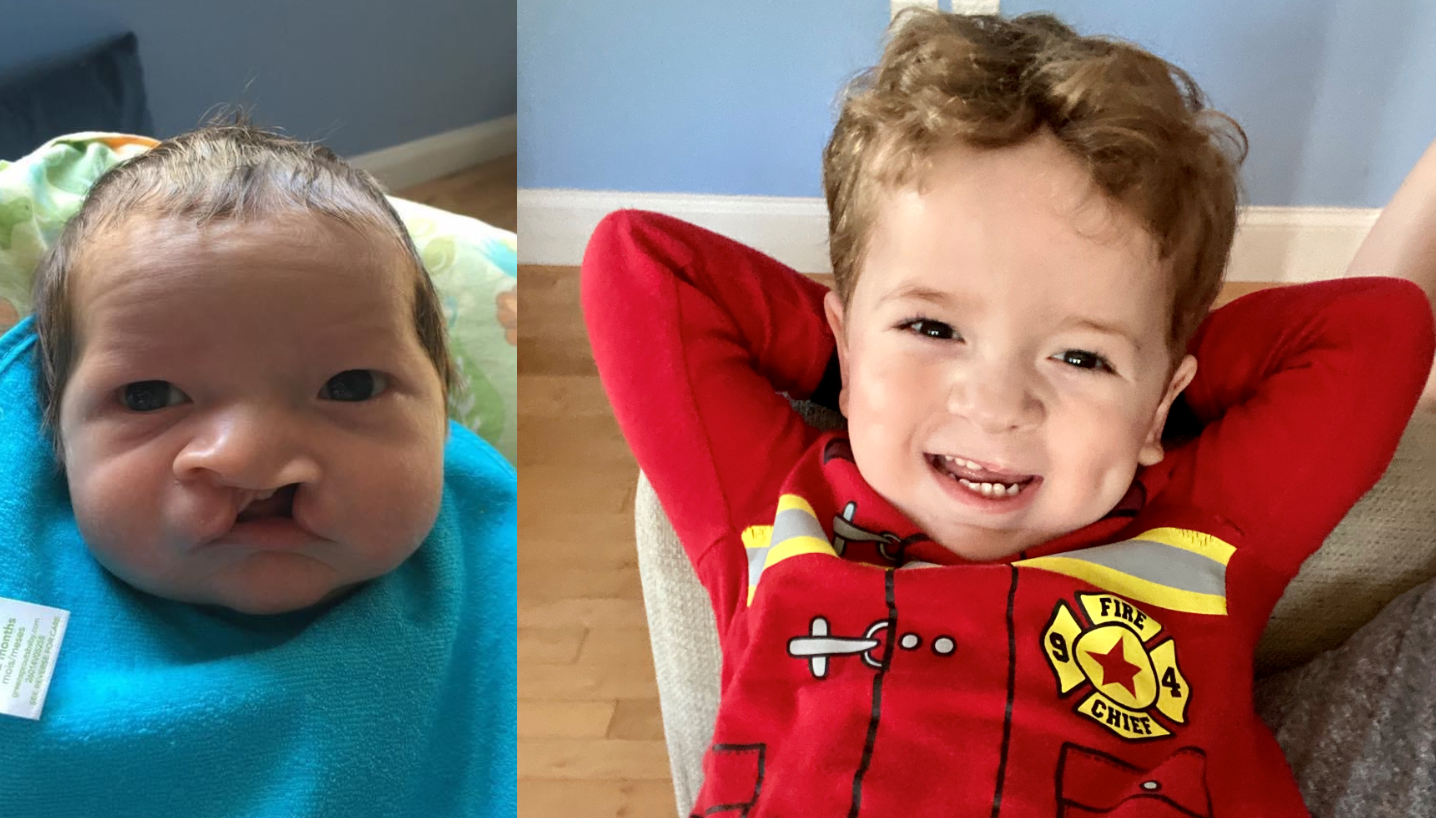
Unilateral complete cleft lip and palate before repair (left) and after nasal molding with DynaCleft, alveolar correction with a Latham appliance, single-stage cleft lip repair, and cleft palate repair.
Although some children need to have another procedure on their lips and/or nose before they begin school, or as they enter adolescence, other children never need further surgery.
Children whose cleft lips involve the alveolus, or gum line, typically need another operation to help their permanent teeth come in and to make it easier for orthodontic treatments to improve their bite and jaw function. This operation is called an alveolar bone graft, and is usually performed when the child is 8 to 10 years old.
Surgical repair: Cleft palate
A plastic surgeon brings together the separated muscles and tissue from the two halves of the palate to close the opening. This procedure is performed in the operating room under general anesthesia. Your child will be in the hospital anywhere from one to three nights after the operation.
A cleft palate is typically closed between the ages of 9 and 11 months, before a baby makes their first attempt to use words. Your child's plastic surgeon will discuss the best repair plan for their needs and circumstances.
Immediately after surgery, you should give your child liquid foods, such as stage 1 baby food, using the side of a soft-tipped baby spoon. After around 10 days, your child will be able to have soft foods, such as stage 3 baby foods or soft cut up fruit. Your surgeon may ask you to rinse your child's mouth with water for the first 10 to 14 days after surgery to help keep the stitches clean.
Your child may regurgitate some food and liquid through their nose for up to three months after the operation. This is normal. It takes time for the swelling to go away and for the muscles in the palate to begin working properly. You'll be given further post-operative instructions when your child is discharged.
Approximately five to 15 percent of all children who have undergone a cleft palate repair will need a second operation to correct “nasal”-sounding speech. These operations are often performed around 4 to 6 years old. A common procedure is called a pharyngeal flap, but other operations may be recommended based on your child’s anatomy.
Long-term monitoring and follow-up
The follow-up care your child will need depends on the extent of his cleft lip and/or cleft palate. In our Cleft Lip and Palate Program, we see patients as frequently as every six months to every other year, from infancy all the way through adolescence.
Your treatment team will develop a follow-up schedule that works best for you, your child, and your family.
How Boston Children's Hospital approaches cleft lip and cleft palate
Boston Children's Hospital treats children with cleft lip and/or cleft palate and the combination through our dedicated Cleft Lip and Palate Program.
Our program:
- is one of the largest in the U.S.
- cares for nearly 900 children and adolescents every year
- uses a multidisciplinary approach that combines expertise in plastic and oral surgery, nutrition, dentistry and orthodontics, otolaryngology, and audiology
- conducts groundbreaking scientific research to better understand the causes of cleft lip and cleft palate, identify new therapies, and work toward finding a cure
Here at Boston Children’s, our compassionate clinicians also understand the emotional and psychosocial toll cleft lip and cleft palate can cause. We recognize your child as an individual — never “just a patient” — and provide vital resources and support to meet the needs of your entire family.
